CODA Craniocervical Dysfunction Initiative (CCD)
The CODA Craniocervical Dysfunction Initiative (CODA CCD) is a research program designed to investigate how structural dysfunction at the craniocervical junction may influence the development and progression of complex chronic disorders.
CODA’s initiative studies craniocervical dysfunction as a biologically anchored model system to better understand the mechanisms that drive complex multisystem illness.
What is Craniocervical Dysfunction?
The craniocervical junction, where the skull meets the upper cervical spine, contains critical neural and vascular structures that regulate autonomic, immune, metabolic, and neurological functions. When biomechanical instability or structural compression occurs in this region, it may disrupt these systems and contribute to widespread symptoms across the body.
Craniocervical dysfunction refers to abnormalities affecting the stability or alignment of the craniocervical junction, These disruptions can alter communication between the brain, spinal cord, and body-wide regulatory systems.
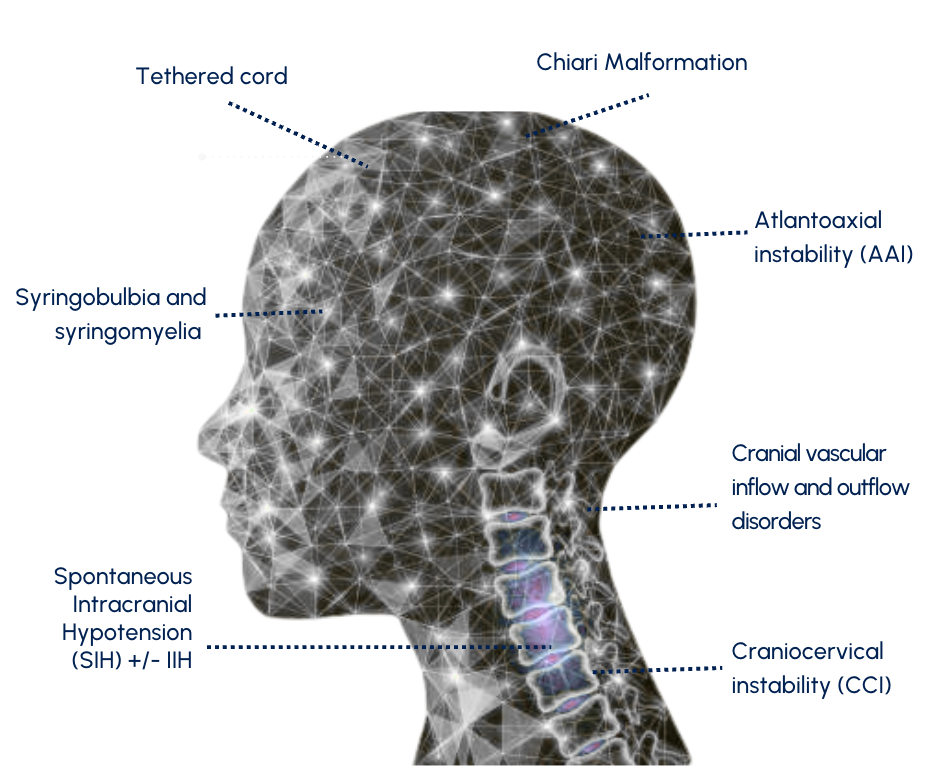
Clinically, patients may receive diagnoses related to craniocervical dysfunction including:
Anatomically Proximal Drivers
Craniocervical instability (CCI)
Atlantoaxial instability (AAI)
Chiari malformation
Syringobulbia and syringomyelia
Cranial vascular inflow and outflow disorders
Anatomically Distal Drivers
Tethered cord
Spontaneous intracranial hypotension (SIH) with or without intracranial hypertension (IIH)
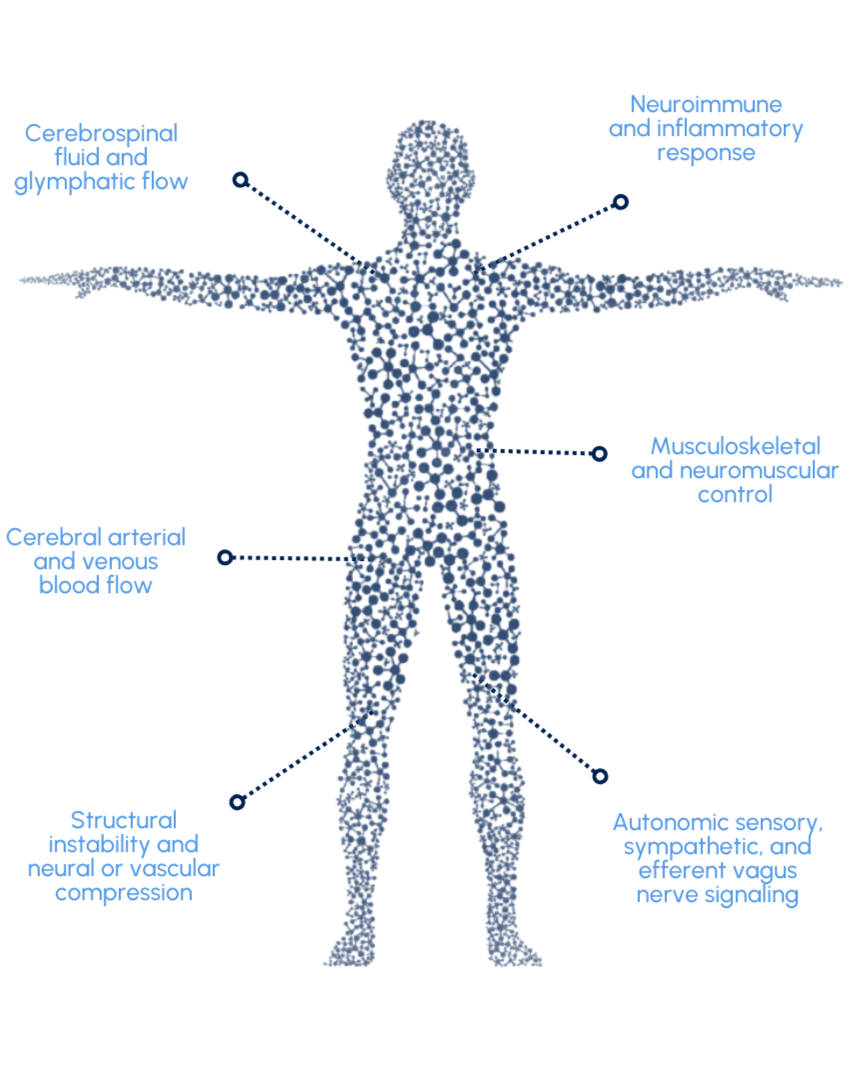
These structural changes may affect key physiological systems including:
Autonomic nervous system regulation
Neuroimmune signaling
Cerebrospinal fluid and glymphatic circulation
Cerebral arterial and venous blood flow
Sensory and vagal nerve signaling
Musculoskeletal and neuromuscular control of the head and neck
Clinically, patients may receive diagnoses related to craniocervical dysfunction including:
Anatomically Proximal Drivers
Craniocervical instability (CCI)
Atlantoaxial instability (AAI)
Chiari malformation
Syringobulbia and syringomyelia
Cranial vascular inflow and outflow disorders
Anatomically Distal Drivers
Tethered cord
Spontaneous intracranial hypotension (SIH) with or without intracranial hypertension (IIH)
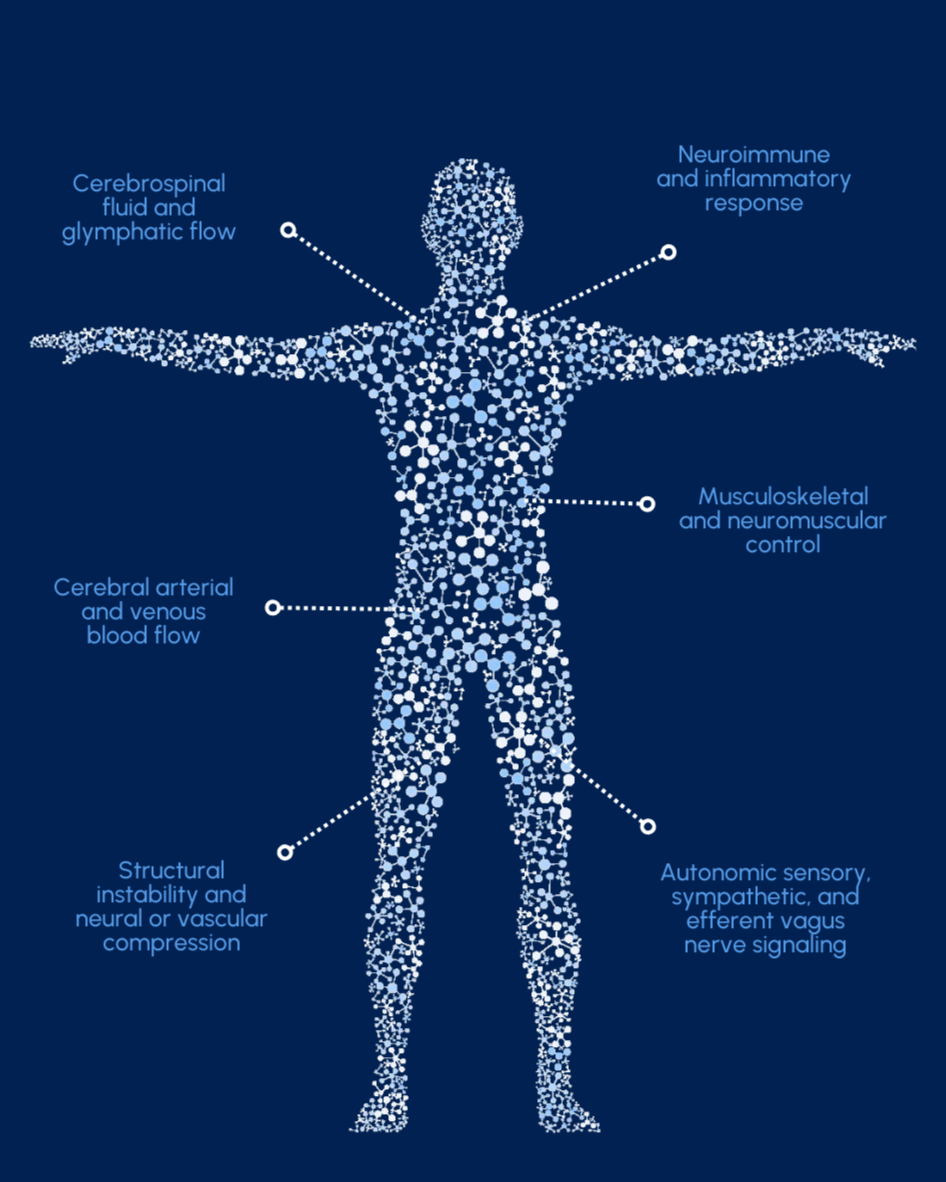
These structural changes may affect key physiological systems including:
Autonomic nervous system regulation
Neuroimmune signaling
Cerebrospinal fluid and glymphatic circulation
Cerebral arterial and venous blood flow
Sensory and vagal nerve signaling
Musculoskeletal and neuromuscular control of the head and neck

Clinically, patients may receive diagnoses related to craniocervical dysfunction including:
Anatomically Proximal Drivers
Craniocervical instability (CCI)
Atlantoaxial instability (AAI)
Chiari malformation
Syringobulbia and syringomyelia
Cranial vascular inflow and outflow disorders
Anatomically Distal Drivers
Tethered cord
Spontaneous intracranial hypotension (SIH) with or without intracranial hypertension (IIH)
These structural changes may affect key physiological systems including:
Autonomic nervous system regulation
Neuroimmune signaling
Cerebrospinal fluid and glymphatic circulation
Cerebral arterial and venous blood flow
Sensory and vagal nerve signaling
Musculoskeletal and neuromuscular control of the head and neck